
The rise of interventional psychiatry, and why it matters for psychedelics
What does it mean, will it live up to the hype, and how could it shape the future of psychedelics?


Big Pharma is showing big interest in psychedelics. In October, AbbVie paid $1.2 billion for a DMT analogue called bretisilocin developed by Gilgamesh Pharmaceuticals, after Gilgamesh reported positive results from a phase 2 trial for depression, with a 94% MADRS remission rate. And at the end of March, Otsuka made a $1.2bn bid for Transcend Therapeutics , after its positive phase 2 trial of methylone, an MDMA analogue, for PTSD.
One reason for the growing interest of Big Pharma in Central Nervous System drugs is the rise of interventional psychiatry as a field. This is a term pioneered by the late Nolan Williams, a psychiatrist at Stanford who did ground-breaking research into Transcranial Magnetic Stimulation and ibogaine. Interventional psychiatry is based on an optimism that mental illnesses that have failed to respond to traditional psychiatric treatments can respond to rapid-acting new interventions like TMS, Spravato and psychedelics.
These are exciting, heady times for the young interventional psychiatry field, with a growing network of academic researchers, a lot of M&A activity, and the chance for psychiatrists to found companies that can be sold for millions.
The rise of interventional psychiatry is also good news for psychedelic drug developers, who feel they have a ready-made infrastructure in which to introduce their treatments. As noted by analysts at Jefferies investment bank, there are well over 5000 clinics offering Spravato across the US, up from 100 in 2019. Jefferies wrote in a note: ‘We estimate greater than 90% of the US population is within less than 25 miles of a Spravato center.’ In addition, there are approximately 2000 clinics offering TMS, and some clinics offering TMS, Spravato and other interventions. ‘This infrastructure should only help facilitate the adoption of future psychedelics,’ notes the investment bank.
Psychedelic drug companies are keen to emphasize their similarity to existing interventional psychiatry treatments and their ‘fit’ with IP clinics. Cybin, a psilocybin drug developer, touted the ecosystem of interventional psychiatry clinics as part of its investment case. Compass Pathways, another psilocybin developer, has announced partnerships with multiple interventional psychiatry clinic chains, such as Radial, Greenbrook and Mindful Health. Both Gilgamesh and Transcend also highlighted these clinics as important to the future of psychedelic medicine. IP clinics are already offering multiple modalities - TMS, Spravato, Biofeedback and so on, soon they may also offer MDMA, psilocybin, DMT, 5meoDMT, LSD and various analogs.
Carey Turnbull, psychedelic philanthropist and founder of two psychedelic drug companies, says:
It’s ironic, if you think of One Flew Over the Cuckoo’s Nest by Ken Kesey. ECT is portrayed in that novel and film as this cruel abusive treatment, while Kesey the Merry Prankster championed psychedelics as the great liberator. Now electrical and psychedelic treatments could be offered under the same roof. In fact, psychedelic treatments were never just about the chemicals, they were also about the synapse activity they triggered.
Robin Carhat-Harris, Ralph Metzner Distinguished Professor in the Department of Neurology at the University of California, San Francisco, comments:
It makes me think of Professor Rupert McShane in Oxford, who started a ketamine clinic out of the ECT clinic in the old psychiatry hospital there. Interventional psychiatry spaces do make sense for psychedelics. I just hope they pay a bit more attention to set and setting than happened in the past with ketamine - the ECT suite at Oxford was not much altered aesthetically, to my knowledge, to accommodate ketamine.
Psychedelics are, of course, non-specific amplifiers of context, and psychedelic experiences are profoundly shaped by the different contexts in which they’re taken - Amazon retreat, underground rave, psychedelic church. How will they interact with the setting of interventional psychiatry clinics?
Historical background for rise of interventional psychiatry
15 years ago, Big Pharma stopped investing in new psychiatric or Central Nervous System drug research. In 2010, GSK, AstraZeneca, Pfizer, Merck and Sanofi all announced they had stopped looking for new antidepressant drugs. Professor David Nutt declared this the “annus horribilis” for psychiatric drug research. Why did Big Pharma pull out of brain drugs? There were too many trial failures, too many adverse events, the placebo effect cast doubt on efficacy, and there was no common theory of mental illnesses. Plus there was easier money to be made in other areas, like cancer drugs.
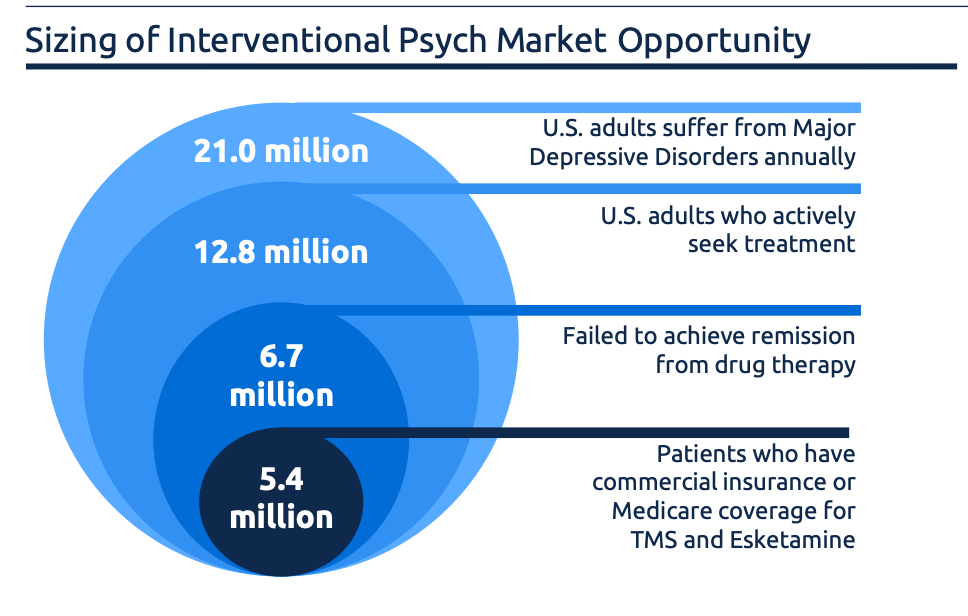
But there was still a big need for better treatments for mental illnesses. Edgemont Research estimates there are 60 million US adults with a mental illness, and only half seek treatment. The standard psychiatric treatments are SSRIs or anti-psychotics, and talk therapy. But these treatments don’t work for a lot of people - an estimated 30-50% of people diagnosed with depression don’t respond to two treatments, classifying as experiencing ‘treatment-resistant depression’. Similar rates of people with PTSD don’t respond to conventional treatments.
In the last few years, Big Pharma has returned to the CNS field. They’re not necessarily funding research themselves (although sometimes they are - Johnson & Johnson / Janssen funded the development of Spravato). More typically, Big Pharma is letting smaller companies take the initial risk with drug or device development, then buying them up if they look promising. Some recent deals include Bristol Meyers Squib buying schizophrenia-drug developer Karuna Therapeutics for $14 billion in 2024, and AbbVie’s $8.4 billion acquisition of schizophrenia drug maker Cerevel in 2023 (its lead drug then failed a Phase 2 trial, underlining the continued risk of the CNS sector).
Part of Big Pharma’s growing interest in CNS treatments is the buzz around interventional psychiatry and its suite of rapid-acting treatments for mental illness, including psychedelics. So what’s the history of the term ‘interventional psychiatry’? It owes a lot to Nolan Williams, the pioneering psychiatrist who tragically passed away last year.
What is interventional psychiatry ?
The term ‘interventional psychiatry’ was introduced by Yale University in 2009, to refer to rapid-acting psychiatric procedures for mental illness such as Trans-Cranial Magnetic Stimulation (TMS) and ketamine. Yale New Haven Psychiatric Hospital launched its interventional psychiatry service in 2013. In 2015, the term was announced to the field in an open letter from psychiatrists at Medical University of South Carolina, lead-authored by Nolan Williams. The authors announced:
Unlike cardiology, radiology, and neurology, the field of psychiatry does not formally recognize or train ‘interventionalists’ who perform specialized procedures on the spectrum between standard care and surgery. The purpose of this letter is to explain why the field of interventional psychiatry should be recognized as a formal subspecialty of psychiatry and further developed…Interventional psychiatry is an emerging subspecialty that utilizes neurotechnologies to identify dysfunctional brain circuitry underlying psychiatric disorders and apply brain stimulation techniques to modulate that circuitry.
Ben Spielberg is a neuroscience PhD and founder of Bespoke, a chain of interventional psychiatry clinics that’s now part of Stella Mental Health. He says:
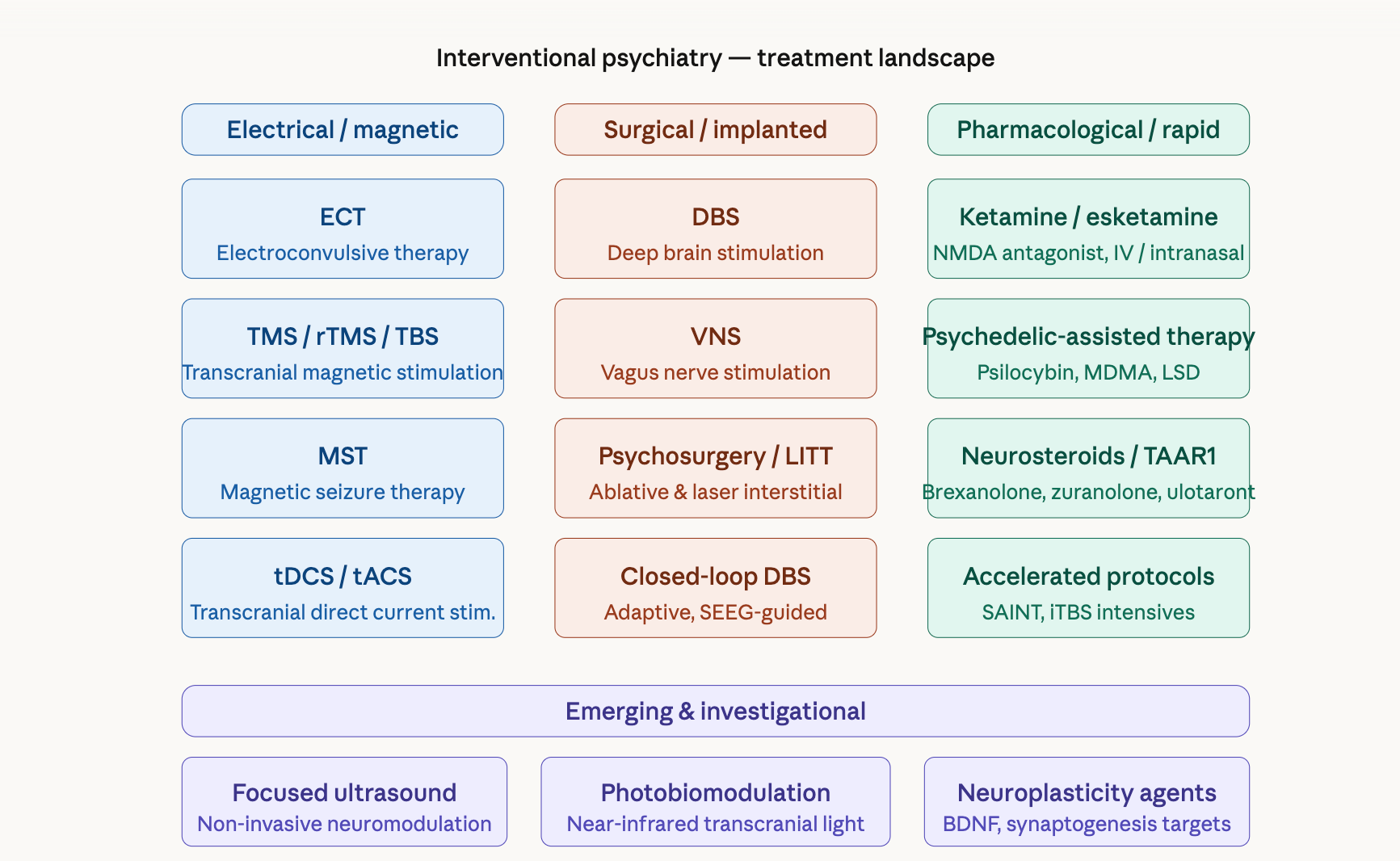
It’s the difference between routine care and procedures. Routine care in psychiatry would be psychotherapy and medication management. Interventions would include electroconvulsive therapy (ECT), TMS and all of its variations, as well as ketamine, and potentially psychedelics.
Grant H. Brenner is an interventional psychiatrist and the founder of Brighter Neurotherapetics. He says: ‘If you think about it, everything a psychiatrist does is interventional. So some of it is branding and marketing. But one way to think of it is procedural psychiatry. Does it involve a procedure that it takes training to give?’
Jeffrey Zabinksi is Director of Interventional Psychiatry at Columbia University Irving Medical Center. He says:
From my vantage point, it looks like so many parallel processes going on, and I’m really curious how they’re going to coalesce. I’m wondering if interventional psychiatry might be a good forum for those things to come together. I don’t know necessarily if it will be, but I suspect it could be a powerful uniting place. But there are some really diverse groups out there - there are people who are doing what I consider interventional psychiatry, who would not consider themselves interventional psychiatrists. There are many people who are very much into brain stimulation, but they don’t think psychedelics should be included. So it’s quite diverse.
What’s on the menu?
The intervention at the core of ‘interventional psychiatry ’ is TMS. This originated in Electro-Convulsive Therapy (ECT), based on discoveries made a century ago. ECT got a bad rap in part because of short-term memory loss, in part because of One Flew Over the Cuckoo’s Nest. Nonetheless, some patients with severe depression found and still find it helpful - including Julian Huxley, Aldous’ brother. In 1985, Anthony Barker at Sheffield University discovered the ability to introduce an electrical current into the brain in a gentler and less painful fashion, using magnets. In the 1990s and early Noughties, researchers including Mark George of Medical University of South Carolina researched using repetitive pulses from a TMS handset to relieve depression. This led to the first FDA clearance of a TMS device for depression in 2008 - the Neurostar TMS machine. George also researched Vagus Nerve Stimulation for depression, which was FDA-cleared in 2006. Meanwhile, one of Mark George’s PhD students - Nolan Williams - developed the SAINT accelerated TMS protocol, trying to do in a few days of intense treatment what had previously taken a few weeks. This was FDA-cleared for treatment-resistant depression through a company called Magnus Medical in 2022. In addition, a company called BrainWay developed a ‘deep TMS’ device, which was cleared by the FDA in 2025.

The response rate for standard TMS for depression is around 50%, with 30% remission rates, while the SAINT accelerated TMS protocol initially reported 86% remission rates, which caused a big stir at the time, although this has since fallen to 50% in replication studies.
Interventional psychiatrists are very excited by the potential of TMS for depression, and also perhaps for other brain conditions, such as Alzheimer’s. They also feel TMS deserves more attention but hasn’t received it yet because it doesn’t have the hype factor that psychedelics do (there is no Netflix documentary about TMS, no Michael Pollan best-seller, no cultural movement, although a few celebrities like Tim Ferriss and Demi Lovato say they’ve found it helpful for depression). Grant Brenner says: ‘TMS really outperforms anti-depressants, it probably outperforms psychedelics, and it’s almost certainly safer and has fewer side effects.’
Ben Spielberg recalls working as a TMS technician:
The population we would see were people who had tried dozens and dozens of medications, and been in therapy for decades, and nothing had worked. I remember the first patient I treated, you could see the depression in their face and movements. After a couple of weeks of TMS, I made a joke, and he started laughing for the first time. Over the next weeks, he completely changed. He started working again. He started feeling happy again. He developed healthier relationships. It was a light-bulb moment.
An even more popular treatment offered by interventional psychiatry clinics is Janssen’s esketamine nasal spray, Spravato. Ketamine has a long history, and was approved by the FDA as an anaesthetic in 1970, but it started to be investigated as a rapid-acting treatment for depression in the Noughties, particularly by the interventional psychiatry team at Yale. Around 2015, clinics started popping up offering IV ketamine infusions for depression and a host of other issues, some run by psychiatrists, others by nurses or anesthetists. There are now hundreds of ketamine clinics, as well as at-home ketamine providers. It’s a Wild West, there’s no agreed protocol, no tracking of adverse events, and not always much warning of the addiction potential of ketamine (something Nolan Williams warned of in a paper noting ketamine binded to opioid receptors in the brain).
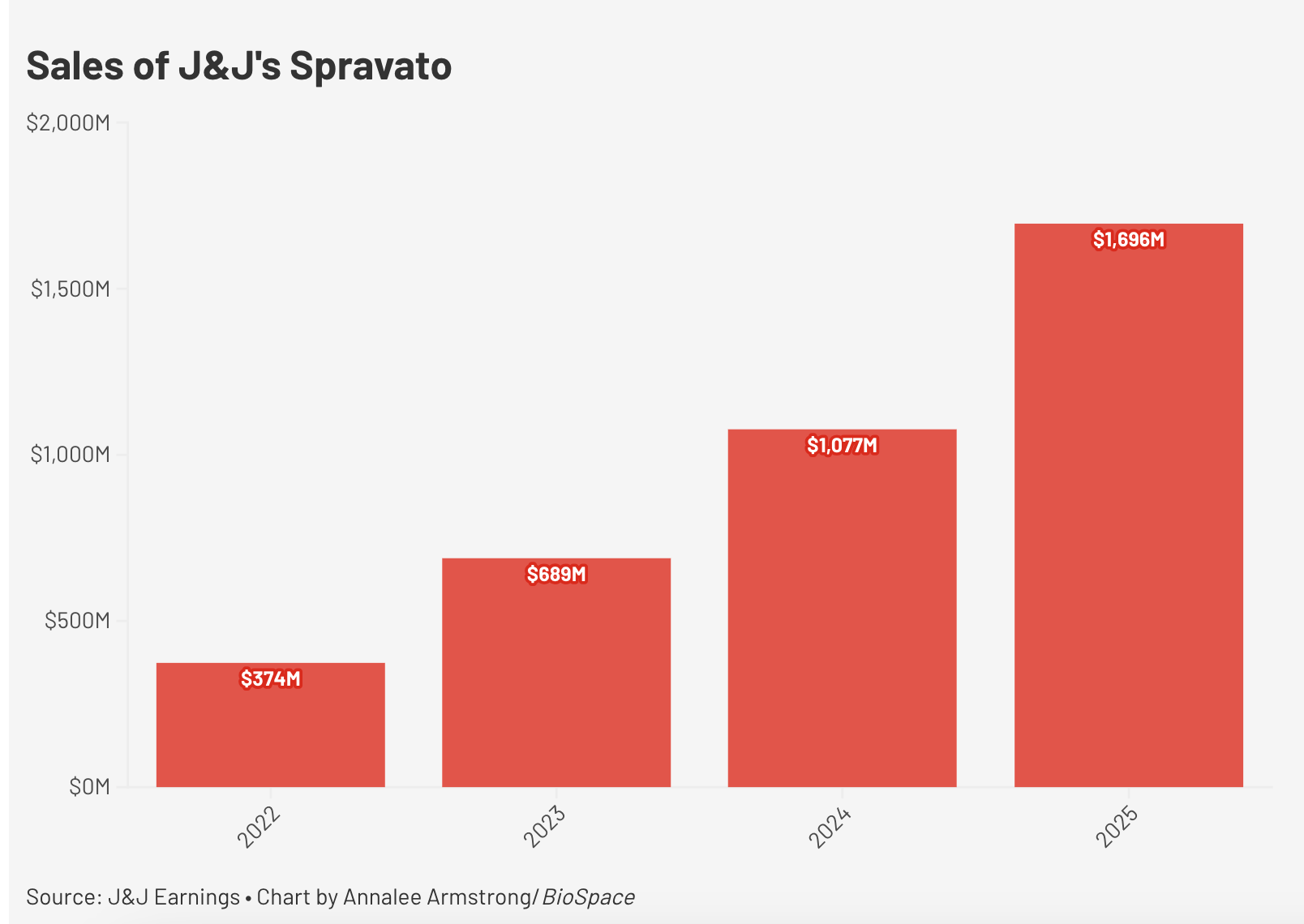
In 2019, Janssen got an esketamine nasal spray called Spravato approved by the FDA for depression. Unlike off-label ketamine, it’s insurance-covered, and is now offered in somewhere between 5000 and 6000 clinics in the US, with 200,000 patients treated so far, and is making Janssen $2 billion a year.
Owen Muir, co-founder of Radial Health, which is a network of interventional psychiatry clinics, says:
Janssen did heroic work with Spravato. My regard for them is tremendous. What they proved was, it’s possible to have a novel treatment with a rapid onset. TMS may actually be more rapid, empirically, but they had a new way of delivering a new mechanism that wasn’t an SSRI. And they got that to scale, with only 600 sites meaningfully prescribing the majority of the volume. So that’s financially successful, and replicable.
Then there are other treatments like Deep Brain Stimulation, focused ultrasound, Stellate Ganglion Block and biofeedback. Typically, these interventions require training and a clinic to give them, but now there are home-use appliances for TMS (like the Flow headset) and for Vagus Nerve Stimulation (the GammaCore device) and ‘home-injectables’ for ketamine.
Circuit theory of mental illness
If there is a theory that connects the various treatments found in interventional psychiatry, it’s the circuits theory of the brain and mental illness: that, in essence, many mental illness are best understood not as chemical imbalances, nor cognitive distortions, existential crises or socio-economic challenges, but as problems in circuit connectivity in the brain.
After the paywall, how will psychedelics fit into the cultural setting of interventional psychiatry, and what are the ethical risks?
