
Belser and Brennan on the EMBARK model
And what they think existing models of psychedelic-assisted therapy leave out

Dr Alexander Belser of Yale and Dr Bill Brennan - psychologist and psychedelic research consultant - both worked at Cybin, a company developing psilocybin-assisted psychotherapy for depression. There, they assessed over 17 models of psychedelic-assisted psychotherapy (PAT) and came up with what they think is the most comprehensive - the EMBARK model, which can be used by both licensed psychotherapists and psychedelic guides or facilitators. They lay out the model out in a new book, out next year, and in a free online course. I interviewed Bill and Alex to ask what they think existing models of PAT are missing, and we dived into the juicy questions of how to incorporate the spiritual, and even the political, into PAT, plus how to make it more ethically-sound. The first half is free to all, second half and the video of our conversation is only for paid subscribers. This is a very helpful interview if you are training to be a psychedelic therapist or facilitator.
Jules Evans: Could you begin by telling me about you?
Alex Belser: My name is Alex Belser. I'm a psychologist. I live in Brooklyn in New York. I'm passionate about therapy and psychotherapy and working with other clinicians trying to alleviate human suffering. My specialisation has been psychedelic medicine. I co founded the psychedelic research project at NYU in 2006, and have been involved in clinical trials as an investigator there, and then later at Yale, to treat depression, alcohol use disorder, anxiety, cancer distress, as well as obsessive compulsive disorder I’m at Yale right now in a team led by Dr. Ben Kelmendi. I've also a Maps therapist, maps just applied for its NDA today for MDMA-assisted psychotherapy, and I have been focusing on the treatment of LGBTQ folks and the queer community and co-authored a recent book Queering Psychedelics, which came out last year, and is looking at the cultural and medical intersections between lineages of the queer community and various forms and diverse forms with psychedelic practice and medicine and consciousness. was the Chief Clinical Officer at Cybin, and with a team of people developed EMBARK as a new integrative model for psychedelic treatment. Bill, you want to go ahead?
Bill Brennan: Sure. I'm Bill Brennan, a psychologist and psychotherapist in Queens, New York. And I got interested in psychedelics in 2003, when I first took them. I met Alex around that time, too. And I became secondarily interested in psychology and psychotherapy because I thought that was the route that psychedelics were going to take into our culture, and that seems to be the case. I was going down that path, wanting to be a psychedelic researcher, but I became a little disenchanted with how psychotherapy is practised in our culture and the way it's not really responsive to the actual conditions that exacerbate or create a lot of the suffering that we frame in terms of medicalized diagnoses. So, I left the field for a little bit and got involved in organising and activism. At some point, I lived in Brazil for a while studying an anarchist somatic psychotherapy called Soma, which I found really interesting. I had hoped to bring it back to the US and practice it here. But it just didn't quite fit in a lot of ways culturally. So, I started to turn my attention back towards psychedelic therapy again in 2015.
And I started to really feel into the potential that's there. It feels like the story is still far from written. We don't really know where it's going to go. So, I started to wade back into the waters and regained some faith in psychedelics and psychotherapy. And around that time, I reconnected with Alex, and he invited me into Cybin. And I've served as a clinical consultant there. I've also worked with Gilgamesh and some other entities in the field. I’ve mostly helped with writing the treatment manuals for trials, providing facilitator training, and clinical supervision.
Jules Evans: Alex, you said you started working in 2006 on psychedelic drugs. So that must be very early in the psychedelic renaissance?
Alex Belser: My first psychedelic conference was in 2001. And it was really a different scene, it was edgier, much more esoteric, there was mostly underground practitioners and you know, some of the psychedelic grandparents of the field were there like Sasha Shulgin and Stan Grof, Alex and Alysson Grey, Rick Doblin etc. In 2006, when we wanted to start a psilocybin trial at NYU, I was a grad student, a junior member of the team. And it took quite a bit of politicking to persuade the members of the IRB, the oncology boards, the general research committees of the university to allow the re entry of psychedelic medicine into the field. It took substantial amount of savvy on the part of people like Steve Ross and Tony Bossis and Jeff Guss to make that happen. And today, the Overton window has shifted - we just have had a geometric explosion in the number of clinical trials that are being registered, and every academic centre in the world wants to have a centre for psychedelic research of some sort at this point. It’s actually quite gratifying, in many ways. And it's also been head spinning to see how much the field has changed.
Jules Evans: So before I ask you to lay out the EMBARK model, could you tell us a bit about Cybin?
Alex Belser: Cybin is a company that's just reported on the results of a phase two trial, investigating CYB 003, which is a deuterated psilocybin analogue for the treatment of depression, specifically major depressive disorder. And not just MDD, but people with major depressive disorder who are also what are called non optimal responders. So they're already on SSRIs, or SNRIs, they may not have full blown treatment resistant depression, meaning they failed to respond to two or more previous treatments, but they're also not firstline people with major depressive disorder. So these are people who have already not responded to or failed out of at least one treatment or not responded to multiple treatments. And the results are really wonderful. We see four out of five people in that trial receiving CYB 003 in conjunction with the EMBARK facilitation, achieving full remission from depression, an average of a 17-point drop on the modulus, which is a clinical gold standard measure of depression. Cybin is where I worked for some time, I'm now doing a little bit of consulting with them. And Bill has been doing some supervision and teaching in the EMBARK model.
Because of Cybin’s willingness to put some resources into EMBARK, we were able to speak with literally over 50 different consultants, leaders in the psychedelic field, teachers, everyone from pharmacists and chemists, to people focused on psychotherapy and clinical research, to learn from what had been done and really take a deeper dive into the literature. We published a few papers on systematic analyses of psychotherapy in psychedelic work and put together a new approach that took what we hoped were some of the best learnings from what happened in previous psychedelic research, but also addressed some of the major gaps in this.

Jules Evans: Could you explain the EMBARK acronym for us?
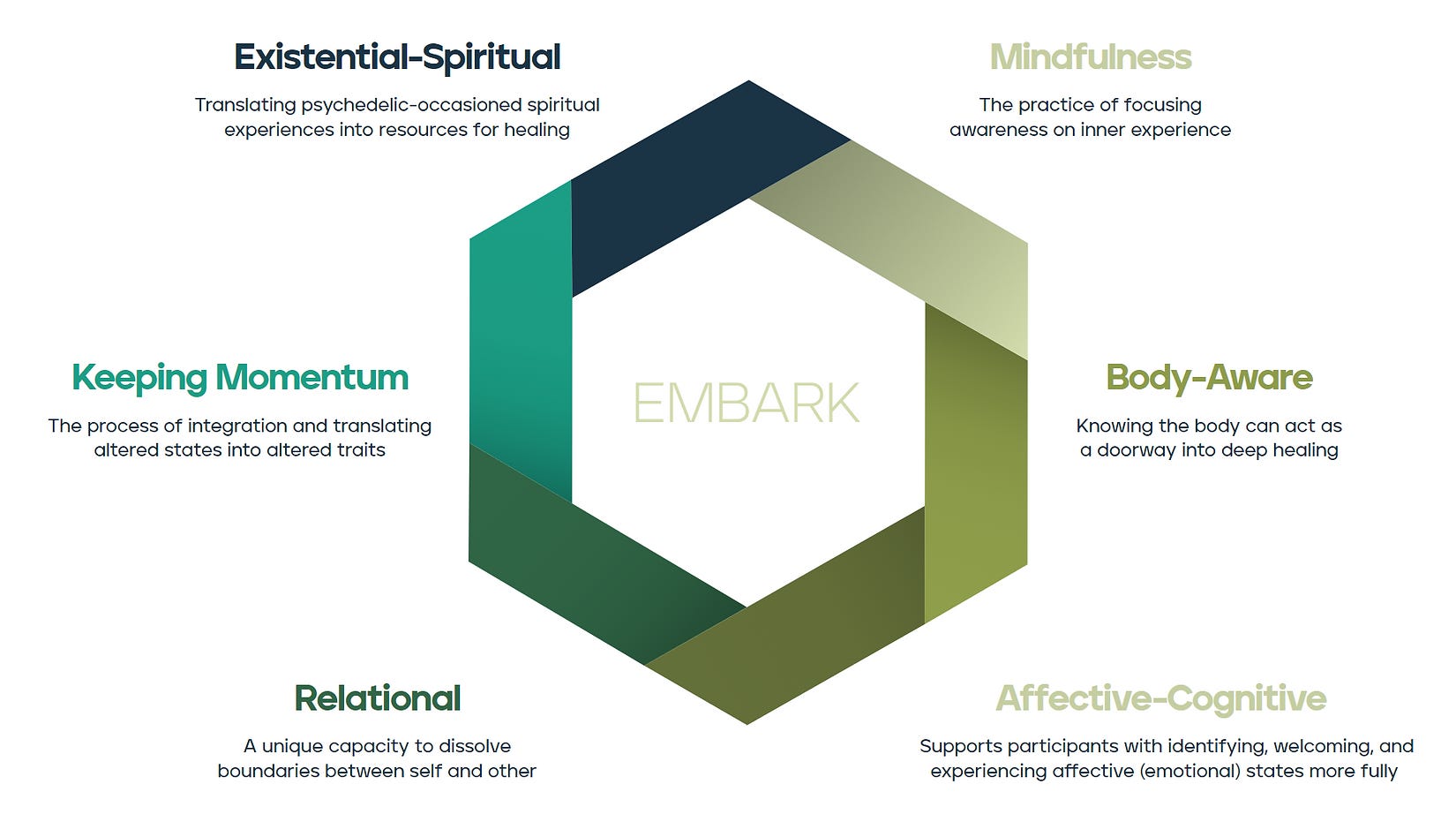
Bill Brennan: Sure. EMBARK consists of the six clinical domains that make up the core of the model. We’ll get into what each of those six clinical domains means in a moment. But at the heart of EMBARK is a respect for the possibility that there are multiple paths to healing, that there are as many paths to healing as there are people undergoing psychedelic treatment. It avoids the pitfall of applying a single unified theory of how treatment works to every single participant experience and instead includes a multiplicity of possibilities for how somebody's treatment experience might evolve. And the six clinical domains that make up the acronym represent the spectrum of parallel pathways to healing that may or may not be important for any given individual participant.
The acronym stands for:
Existential spiritual
Mindfulness
Body aware
Affective-cognitive
Relational
Keeping momentum
So just a brief summary what each of those means.
E – the Existential-spiritual domain – includes encounters with any kind of religious, spiritual, mystical, existential content, any of the big picture material, encounters with spiritual entities, or all the things that are typically thought of as mystical experience.
M - Mindfulness refers to any kind of psychedelic-elicited experience that involves a shift to one's sense of self, or relationship to self, or the relationship to the workings of the mind. So, anything that allows a participant to have more of a mindful, removed perspective on what's going on, whether it's rumination with depression, or cravings with a substance use disorder. Having a bit more of that mental freedom.
B - the Body-aware domain - refers to the fact that psychedelic experiences are deeply embodied. A lot of times people report healing experiences going on in their body that aren't primarily psychological or mental and maybe don't even map onto any kind of mental phenomena. We want to respect the body as a potential primary site of healing that operates in and of its own logic.
A - Affective cognitive – This is the bread and butter of traditional psychotherapy, emotions and core beliefs, where people can have big affective openings, experiencing things like grief or joy, to an extent to which they don't normally have access. And there might be a transformation of those emotions and the core beliefs that accompany those emotions. This domain creates a space in the model for that.
R – the Relational domain. We typically have thought of psychedelic treatment as a kind of “one person psychotherapy” where the participant goes inside, and they're focused on the music, they've got the eyeshades on, they're having this very personal experience. But we found that a lot of times people take off the eyeshades, they take off the headphones, they're still having a relational experience with other people in the room, the facilitators, the therapists. Even if they keep the eyeshades on, there is still another presence in the room that is impacting the experience. And there's so much potential for healing in these relational aspects if they’re navigated skillfully. We noticed that other models weren't really attending enough to this.
K - the Keeping momentum domain - is a place within the model for recognising that people often go through a kind of self-persuasive process where they're increasing their motivation and their readiness to make changes in their life, whether it's changes in their habits or their behaviours, or in the contexts around them, like their social spheres or their workplaces, and the possibility that they will emerge from treatment feeling really ready to do that.
Jules Evans: You said you surveyed the field - what are the main existing models of PAT and what are they missing?
After the paywall, incorporating the relational, the spiritual and the political into PAT, and how to put ethics at the heart of it.
